

It was 1968. Dr. Rosenberg witnessed an extraordinary case in which a patient’s immune system had vanquished cancer. Hoping there was an elixir in the man’s blood, Dr. Rosenberg got permission to transfuse some of it into a patient dying of stomach cancer. The effort failed. But it was the beginning of a lifelong quest.
Now, versions of the therapy for a limited number of blood cancers are nearing approval by federal regulators, and could reach the market as early as next year.
The technique, known as cell therapy, gives each patient an individualized and souped-up version of their own immune system, one that “works better than nature made it,” as Dr. June puts it.
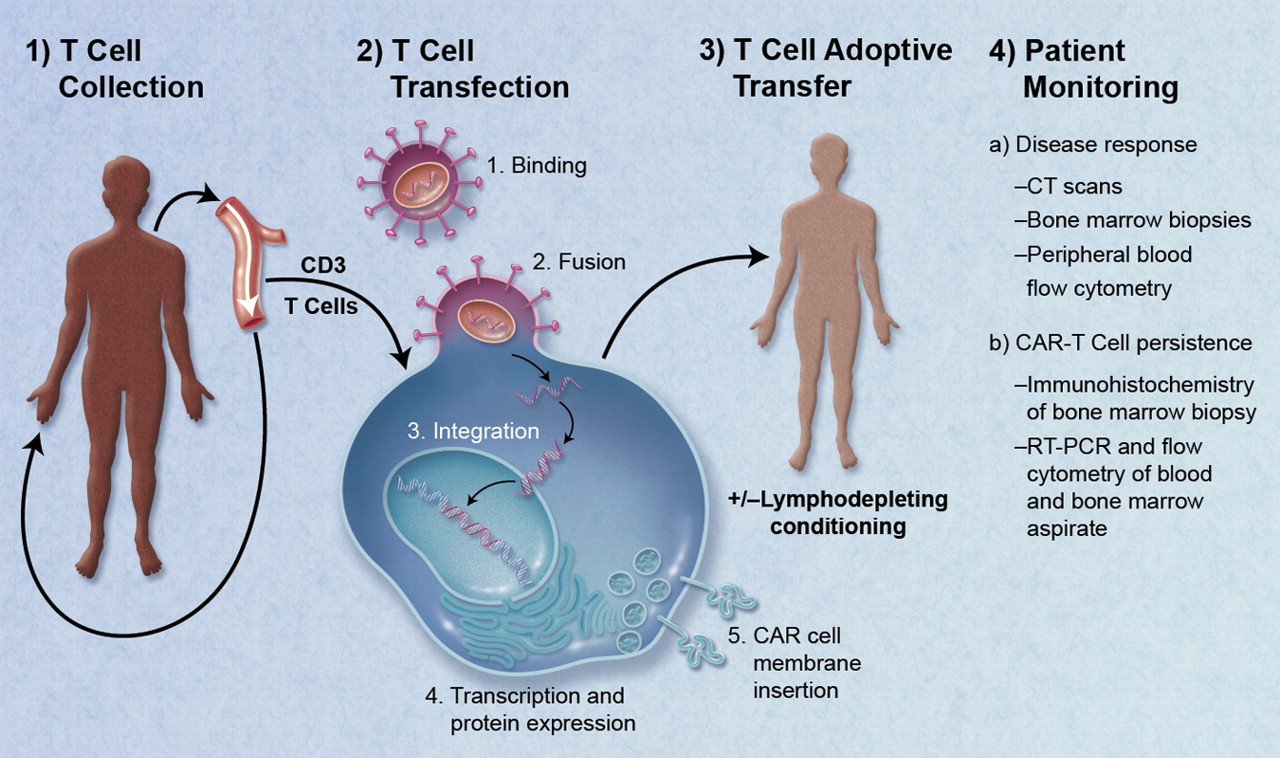
The patient’s T-cells, the soldiers of the immune system, are extracted from the patient’s blood, then genetically engineered to recognize and destroy cancer. The redesigned cells are multiplied in the laboratory, and millions or billions of them are put back into the patient’s bloodstream, set loose like a vast army of tumor assassins.
This is an unusual pharmaceutical — a drug that is alive and can multiply once inside the body. Dr. June calls these cells “serial killers.” A single one can destroy up to 100,000 cancer cells.
The killer cells are genetically engineered to produce a complex protein, an amalgam of pieces from different parts of the immune system that is unlike anything seen before.
This radical, science-fiction like therapy differs sharply from the more established type of immunotherapy, developed by other researchers. Those off-the-shelf drugs, known as checkpoint inhibitors, release a molecular brake on the immune system, freeing it to fight the cancer much as it fights infections by bacteria or viruses.
Cell therapy, in contrast, is brewed specially for each patient, one of the many challenges the field faces in broadening its use. So far, the number of patients treated with cell therapy is in the hundreds, not thousands. And for now it works only for certain types of blood cancers, not common malignancies like breast and lung cancer. Researchers are also still working out how to control potentially lethal side effects. Just recently, a clinical trial was briefly halted after three patients died of brain swelling.
Still, cell therapy has produced complete remissions in some patients who were out of treatment options, stirring excitement among doctors and patients and setting off a race among companies to bring the treatments to market.
New approaches might allow cell therapy to be used for most patients.
Many other improvements are on the runway.
Dr. Sadelain and Juno are working on “armored CARs” that not only bind to the target but produce immune-stimulating chemicals. Cellectis, a French company, has treated two babies with an off-the-shelf CAR treatment that does not require each patient’s cells to be processed. Bellicum Pharmaceuticals is working on genetic switches that dim or shut off the CAR if the treatment is endangering the patient.
“We’re in the Model T version of the CAR now,” said Dr. Levine, now the director of the cell production facility at the University of Pennsylvania. “What’s coming along are Google CARs and Tesla CARs.”
SOURCE- NY Times

Brian Wang is a Futurist Thought Leader and a popular Science blogger with 1 million readers per month. His blog Nextbigfuture.com is ranked #1 Science News Blog. It covers many disruptive technology and trends including Space, Robotics, Artificial Intelligence, Medicine, Anti-aging Biotechnology, and Nanotechnology.
Known for identifying cutting edge technologies, he is currently a Co-Founder of a startup and fundraiser for high potential early-stage companies. He is the Head of Research for Allocations for deep technology investments and an Angel Investor at Space Angels.
A frequent speaker at corporations, he has been a TEDx speaker, a Singularity University speaker and guest at numerous interviews for radio and podcasts. He is open to public speaking and advising engagements.