

This was a brilliant talk by Joseph Wu, Director, Stanford Cardiovascular Institute. Dr. Wu received his medical degree from Yale and completed his medicine residency and cardiology fellowship training followed by a PhD (molecular pharmacology) at UCLA.
He followed a good act (Dr. Hamati on exosomes) and also showed fantastic repair of heart tissue following injury from a heart attack. But he proposed a model that a) used stem cells and b) could be a massive game changer for drug discovery. He had a few gems so I’ll highlight them here, but he also published amazing articles recently that are certainly worth a read.
Putting The Beat Back On The Heart
 Ladies, listen up: cardiac disease is more common in women than men. Globally, it’s the number one killer, beating out accidents, communicable diseases and cancer. The WHO states that cardiovascular diseases killed 17.5 million people in 2012, that is 3 in every 10 deaths. Of these, 7.4 million people died of ischaemic heart disease and 6.7 million from stroke. So across cultures, the need for preventing heart damage, and rejuvenated injured heart tissue is of utmost importance.
Ladies, listen up: cardiac disease is more common in women than men. Globally, it’s the number one killer, beating out accidents, communicable diseases and cancer. The WHO states that cardiovascular diseases killed 17.5 million people in 2012, that is 3 in every 10 deaths. Of these, 7.4 million people died of ischaemic heart disease and 6.7 million from stroke. So across cultures, the need for preventing heart damage, and rejuvenated injured heart tissue is of utmost importance.
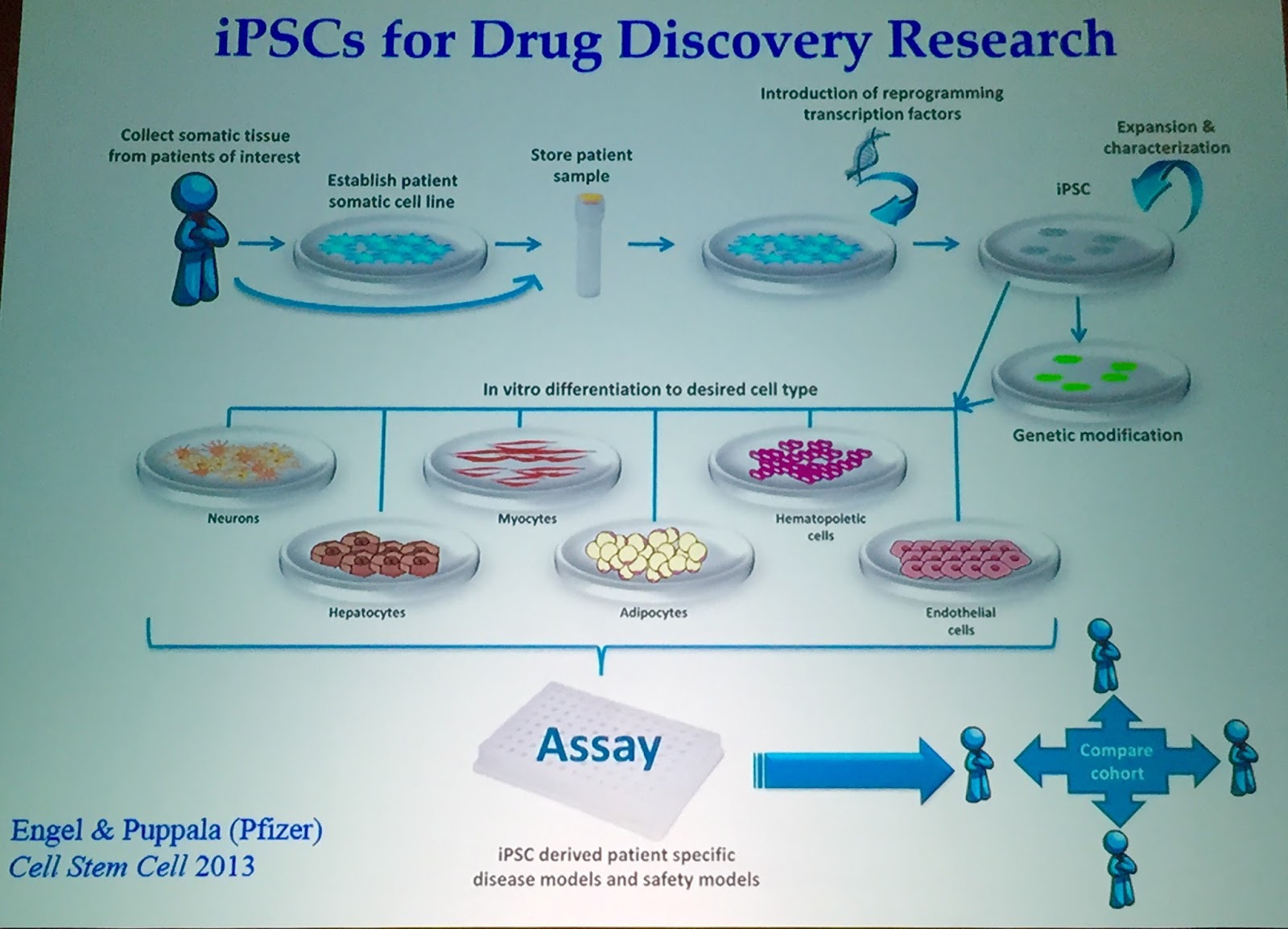
Dr. Wu has been looking at how to take human embryonic stem cells (ESCs) to make cardiomyocytes (cardiac muscle cells) for the past decade. When Nobel prize winner Shinya Yamanaka discovered how to take healthy skin cells (fibroblasts) and turn them into cardiomyocytes, it changed the stem cell game. Now there are quite a few cardiac differentiation protocols out there. About ten years ago, Wu was turning hESCs into cardiomyocytes – but not all the cells twitched like a beating heart. This was a problem for real – and long-lasting clinical outcomes. Fast forward ten years and they successfully made human cardiomyocytes from patient blood – with 90% efficacy. Just think: you can take one cc of blood, make induced pluripotent stem cells (iPSCs) and make millions of beating heart cells!
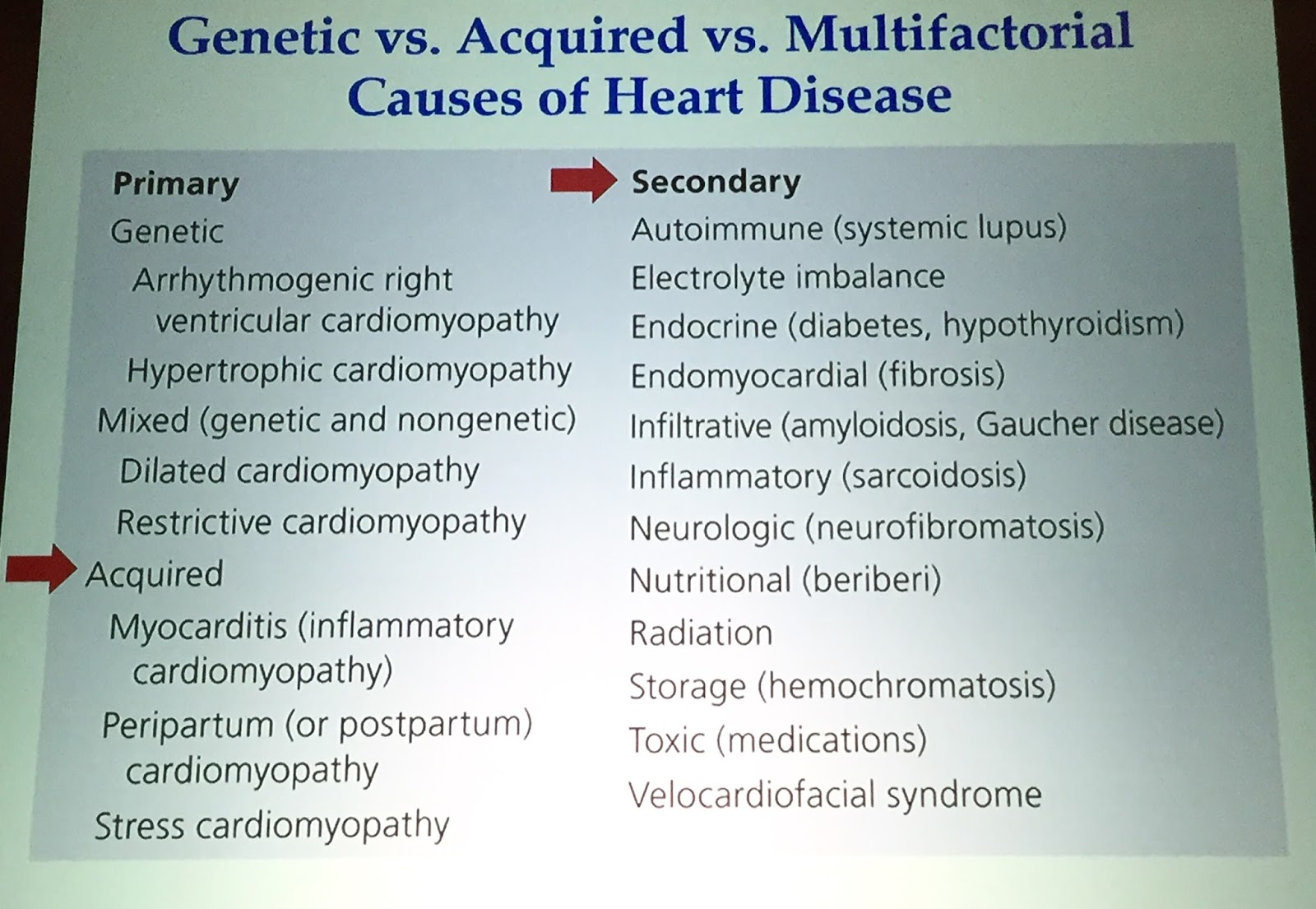
 This opens up the doors to model hard-to-treat heart diseases. For instance, familial hypertrophic cardiomyopathy is the most prevalent inherited cardiovascular disease affecting primarily young people. While you could theoretically use animal cells to treat this, mouse heart beats are so vastly different than human heat beats that it doesn’t translate well. Using iPSCs, Wu’s group was able to recapitulate numerous characteristics of hypertrophic cardiomyopathy. This shows that using these cells is not only a ways to make functional cells for treatment, but also could be a platform for both understanding disease and drug discovery.
This opens up the doors to model hard-to-treat heart diseases. For instance, familial hypertrophic cardiomyopathy is the most prevalent inherited cardiovascular disease affecting primarily young people. While you could theoretically use animal cells to treat this, mouse heart beats are so vastly different than human heat beats that it doesn’t translate well. Using iPSCs, Wu’s group was able to recapitulate numerous characteristics of hypertrophic cardiomyopathy. This shows that using these cells is not only a ways to make functional cells for treatment, but also could be a platform for both understanding disease and drug discovery.
And that’s exactly what they’re up to.
Clinical Trials In A Dish
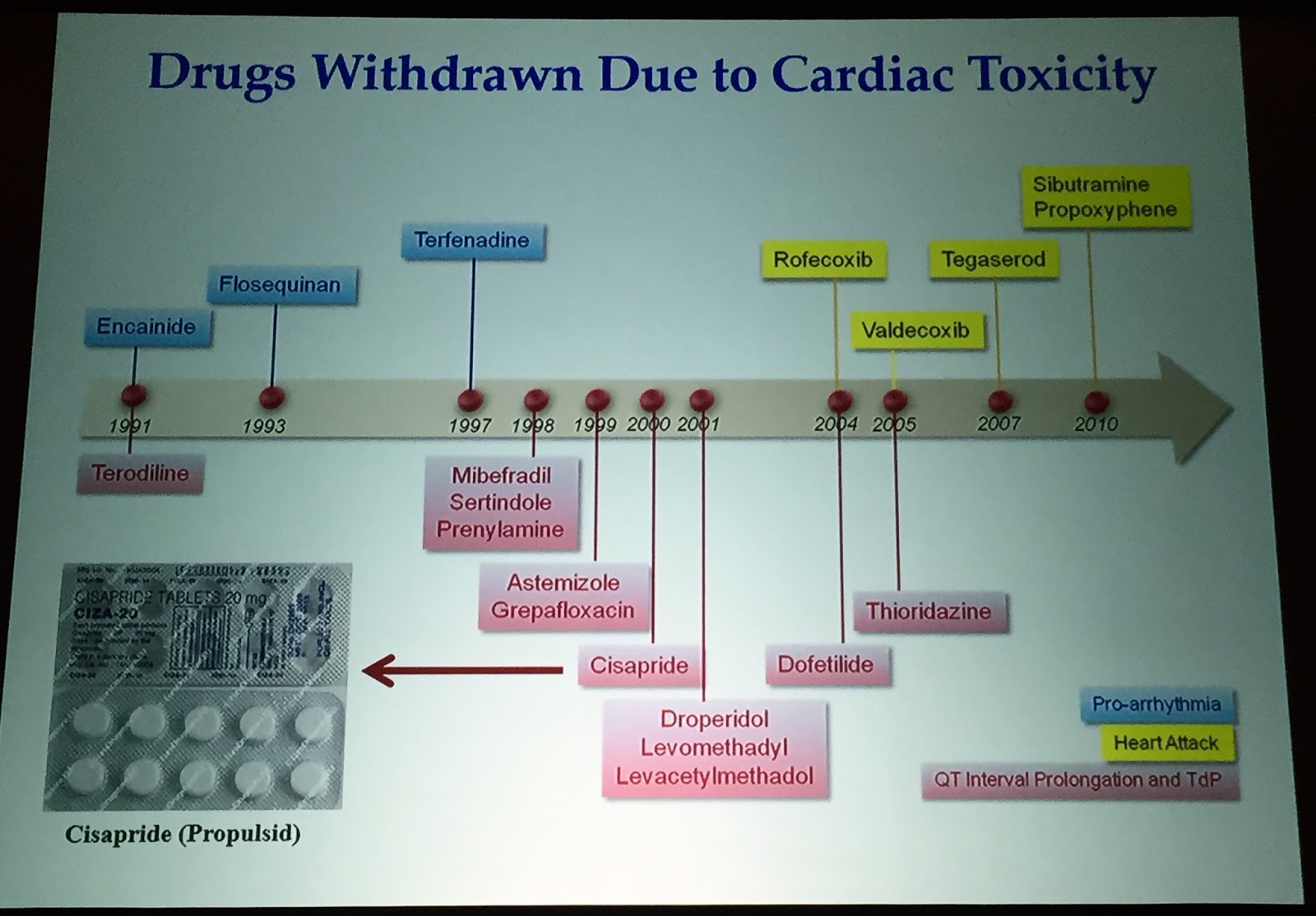
Pharmaceutical innovation is endangered; The image above shows the drugs withdrawn due to cardiac toxicity. Cisapride was even hit with a $90M lawsuit. With more detailed data, scientists could design clinical trials better.
 Another interesting tidbit provided by Wu was on metabolism of alcohol. The ‘asian flush’ experienced by many in this world is known to be a result of an aldehyde dehydrogenase genetic polymorphism. But what’s interesting is that when they get a heart attack, they get it worse than others. And the recovery of the heart muscle is not as salient. In the lab, there is more cell death upon exposure to ischemia. This population is important to understand in the context of heart recovery – and could be a platform for drug testing.
Another interesting tidbit provided by Wu was on metabolism of alcohol. The ‘asian flush’ experienced by many in this world is known to be a result of an aldehyde dehydrogenase genetic polymorphism. But what’s interesting is that when they get a heart attack, they get it worse than others. And the recovery of the heart muscle is not as salient. In the lab, there is more cell death upon exposure to ischemia. This population is important to understand in the context of heart recovery – and could be a platform for drug testing.
Imagine using cells instead of recruited patients to do clinical trials. Using these cells to create a whole library of cell lines that can be manipulated. This is the beginning of personalized medicine.