

The artificial pancreas — a device which monitors blood glucose in patients with type 1 diabetes and then automatically adjusts levels of insulin entering the body — is likely to be available by 2018, conclude authors of a paper in Diabetologia (the journal of the European Association for the Study of Diabetes). Issues such as speed of action of the forms of insulin used, reliability, convenience and accuracy of glucose monitors plus cybersecurity to protect devices from hacking, are among the issues that are being addressed.
1.5 million people in the United States have Type 1 diabetes. The amount of insulin they need at any given moment is always changing — day to day, hour to hour, even minute to minute. Insulin is the hormone that allows your body’s cells to absorb glucose, the gasoline that makes cells go. No insulin, no life.
Three of these academic competitors — Hovorka, Kovatchev and Phillip — have already partnered with companies to commercialize their efforts. Hovorka and Phillip are with Medtronic, the current industry leader in diabetes technology; Kovatchev is with a startup named TypeZero Technologies.
Another competitor Damiano founded a “public benefit” corporation in October, the kind normally used to run transit systems and utilities. The firm, Beta Bionics, quickly secured $5 million in funding from Eli Lilly and Co., the pharmaceutical giant. Damiano serves as CEO but remains a professor at Boston University, where he continues to seek research grants from NIH.
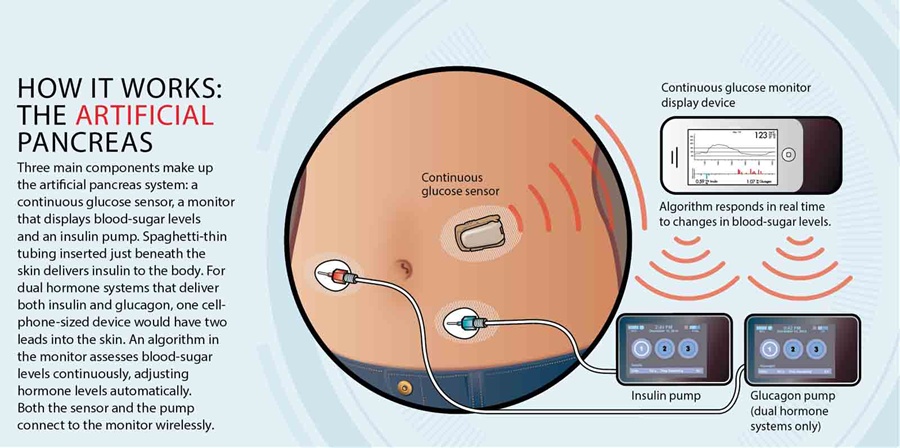
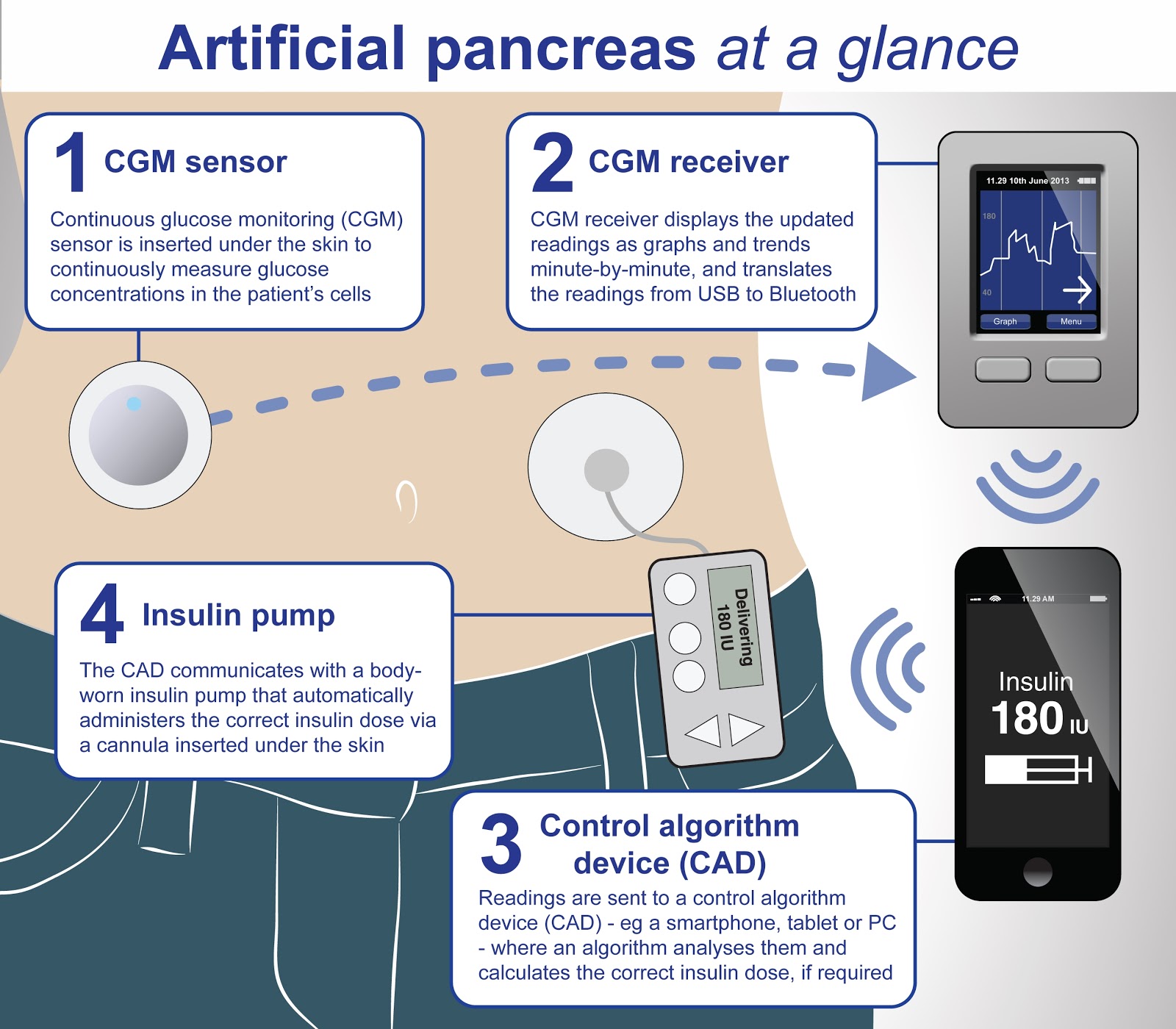
Currently available technology allows insulin pumps to deliver insulin to people with diabetes after taking a reading or readings from glucose meters, but these two components are separate. It is the joining together of both parts into a ‘closed loop’ that makes an artificial pancreas. In trials to date, users have been positive about how use of an artificial pancreas gives them ‘time off’ or a ‘holiday’ from their diabetes management, since the system is managing their blood sugar effectively without the need for constant monitoring by the user.
One part of the clinical need for the artificial pancreas is the variability of insulin requirements between and within individuals — on one day a person could use one third of their normal requirements, and on another 3 times what they normally would. This is dependent on the individual, their diet, their physical activity and other factors. The combination of all these factors together places a burden on people with type 1 diabetes to constantly monitor their glucose levels, to ensure they don’t end up with too much blood sugar (hyperglycaemic) or more commonly, too little (hypoglycaemic). Both of these complications can cause significant damage to blood vessels and nerve endings, making complications such as cardiovascular problems more likely.
There are alternatives to the artificial pancreas, with improvements in technology in both whole pancreas transplantation and also transplants of just the beta cells from the pancreas which produce insulin. However, recipients of these transplants require drugs to supress their immune systems just as in other organ transplants. In the case of whole pancreas transplantation, major surgery is required; and in beta cell islet transplantation, the body’s immune system can still attack the transplanted cells and kill off a large proportion of them (80% in some cases). The artificial pancreas of course avoids the need for major surgery and immunosuppressant drugs.
Researchers globally continue to work on a number of challenges faced by artificial pancreas technology. One such challenge is that even fast-acting insulin analogues do not reach their peak levels in the bloodstream until 0.5 to 2 hours after injection, with their effects lasting 3 to 5 hours. So this may not be fast enough for effective control in, for example, conditions of vigorous exercise. Use of the even faster acting ‘insulin aspart’ analogue may remove part of this problem, as could use of other forms of insulin such as inhaled insulin. Work also continues to improve the software in closed loop systems to make it as accurate as possible in blood sugar management.
A number of clinical studies have been completed using the artificial pancreas in its various forms, in various settings such as diabetes camps for children, and real life home testing. Many of these trials have shown as good or better glucose control than existing technologies (with success defined by time spent in a target range of ideal blood glucose concentrations and reduced risk of hypoglycaemia). A number of other studies are ongoing. The authors say: “Prolonged 6- to 24-month multinational closed-loop clinical trials and pivotal studies are underway or in preparation including adults and children. As closed loop devices may be vulnerable to cybersecurity threats such as interference with wireless protocols and unauthorised data retrieval, implementation of secure communications protocols is a must.”
The actual timeline to availability of the artificial pancreas, as with other medical devices, encompasses regulatory approvals with reassuring attitudes of regulatory agencies such as the US Food and Drug Administration (FDA), which is currently reviewing one proposed artificial pancreas with approval possibly as soon as 2017. And a recent review by the UK National Institute of Health Research (NIHR) reported that automated closed-loop systems may be expected to appear in the (European) market by the end of 2018. The authors say: “This timeline will largely be dependent upon regulatory approvals and ensuring that infrastructures and support are in place for healthcare professionals providing clinical care. Structured education will need to continue to augment efficacy and safety.”
SOURCES- Eurekalert, Discover Magazine

Brian Wang is a Futurist Thought Leader and a popular Science blogger with 1 million readers per month. His blog Nextbigfuture.com is ranked #1 Science News Blog. It covers many disruptive technology and trends including Space, Robotics, Artificial Intelligence, Medicine, Anti-aging Biotechnology, and Nanotechnology.
Known for identifying cutting edge technologies, he is currently a Co-Founder of a startup and fundraiser for high potential early-stage companies. He is the Head of Research for Allocations for deep technology investments and an Angel Investor at Space Angels.
A frequent speaker at corporations, he has been a TEDx speaker, a Singularity University speaker and guest at numerous interviews for radio and podcasts. He is open to public speaking and advising engagements.