

Approaches to achieving radical life extension involve many scientific unknowns. There is uncertainty around whether the different forms of aging damage can be repaired. There is an approach to immortality that replaces scientific unknowns with huge technical challenges.
The technically challenging approach is:
1. Rejuvenate the body by growing a body using an egg cell gene edited to not grow the brain
2. Transfer the rejuvenated brain to the rejuvenated body
3. Connect the brain and restore the spinal cord
4. Rejuvenate the human brain through 6-10 surgeries that each replace 10-16% of the old brain with new young grown brain tissue
The brain surgeries for rejuvenating the brain would be done over 20 years. The brainless body would be grown over about 15-18 years and would need to be on constant life support. The brain surgeries would be causing intentional and planned major strokes which would require recovery, restoration and therapy. Repairing the spinal cord and other problems associated with the brain transfer are discussed in detail in the following paper.
Critical to the success for achieving the end goal (a form of physical immortality) is full recovery from the intentional induced major stroke surgeries and maintaining the identity and personality and consciousness of the individual.
It is vastly difficult. They are talking about a team of surgeons working for about ten hours. Eventually this would require advanced robotic surgery to make it faster, safer, reliable and affordable.
Yes, far from possible NOW. But is it more possible that other approaches to radical life extension? Could it be perfected?
Comparing it to other approaches to radical life extension. Most of the other approaches involve a lot of new science and analyzing very complex processes. We do not know if those other approaches will work. Everything about this approach is something that we have a fairly detailed understanding of the difficulty and the science.
The brain rejuvenation surgeries and processes is discussed at this article and this article which both have videos.
This concept of a brain transplant is an advanced plan based on Dr. Canavero’s who has previous experience with acute spinal cord repair. Canavero and others have proven spinal cord repair in animals from rats to cats, dogs, and monkeys. That work was never believed possible until Dr. Canavero assembled a team of scientists worldwide to solve the many aspects of that achievement. The work was based on a fundamental misunderstanding of the mechanisms involved in spinal neuron regrowth. His revelation that the short neurons regrow to re-establish primitive motor pathways present in species from their origins is a breakthrough in science.
Now, Dr. Canavero is challenging science and humanity with the possibility of a brain transplant. Kidney, liver, lung, hand, heart, and face transplants have all been done in the late 20th century. Yet, the scientific success was delayed in these major advances by the emotional, ethical, and religious objections which were raised. This project of a brain transplant will not doubt undergo similar criticism. Yet, the scientific question remains as to whether such a transplant can be achieved.
BRAVE, the BRain Anastomosis Venture is part of a larger scope project – PERSEUS – that aims at moving an old brain into a young immunoconditioned body (or a nonsentient clone tout court when this becomes available) and kick off rejuvenation of the brain, as afforded by Progressive Brain Replacement (J Hebert, accompanying editorial).
Challenges of Brain Transfer:
1. Impossibility to extract the brain proper from the dura mater, given the intimate relationship between the brain’s venous and cerebrospinal fluid (CSF) outflow and the dural cranial sinuses
2. Impossibility to resuture the internal carotid and vertebral arteries (ICAs/VAs) and the internal jugular veins (IJV) once the brain is laid on the donor’s skull base
3. Lack of an efficient technology to functionally reconnect the 12 pairs of cranial nerves
4. Lack of a technology to reconnect the severed spinal cord
5. Undetermined neuroprotective measures to deploy between the moment of physical separation of the brain from R’s skull and re-establishment of circulation after positioning on D’s skull base
6. Possible immune rejection if BT is carried out on a heterologous body rather than R’s clone.
The last three points are covered elsewhere.
* the spinal cord – once sharply severed – can be functionally reconnected in primates (GEMINI protocol: Fully reviewed in Canavero and Ren)
* Brain protection through profound hypothermia has been demonstrated by Dr. White 50 years ago in primates and more recently confirmed in China. Other techniques can boost hypothermia’s effects. The brain is a partially immunoprivileged organ.
* Brain Transfer on a clone would not require immunosuppressants. Tolerogenic protocols are being developed that may be tapped for heterologous brain transfers.
The Brain is Transplanted Along With the Dural Sac
Sparing the dural venous sinuses along with all the veins and arachnoidal granulations is currently unachievable. Besides, the subdural circulation of CSF would be totally disrupted. The solution is transplanting the brain inside the dural sac.
Briefly, both individuals are trachetomized and ventilated and installed in the upright position. Heads are secured on both sides with a fixation apparatus adapted from the maxillofacial equivalent and centered on the mastoids. A standard fixation is of course to no avail given the wide dural exposition necessary for a BT and the associated ultraextensive craniectomy.
Predicated on the complete expendability of R’s body, the approach in R starts with a nasion-C7 spinous process linear incision followed by full thickness scalping of the head down to the orbital ridges. The skull cap is removed in standard fashion, with multiple burr holes on the two sides of the superior longitudinal sinus and other holes, including along the basal circumference. A standard wide craniectomy frees the cerebellum.
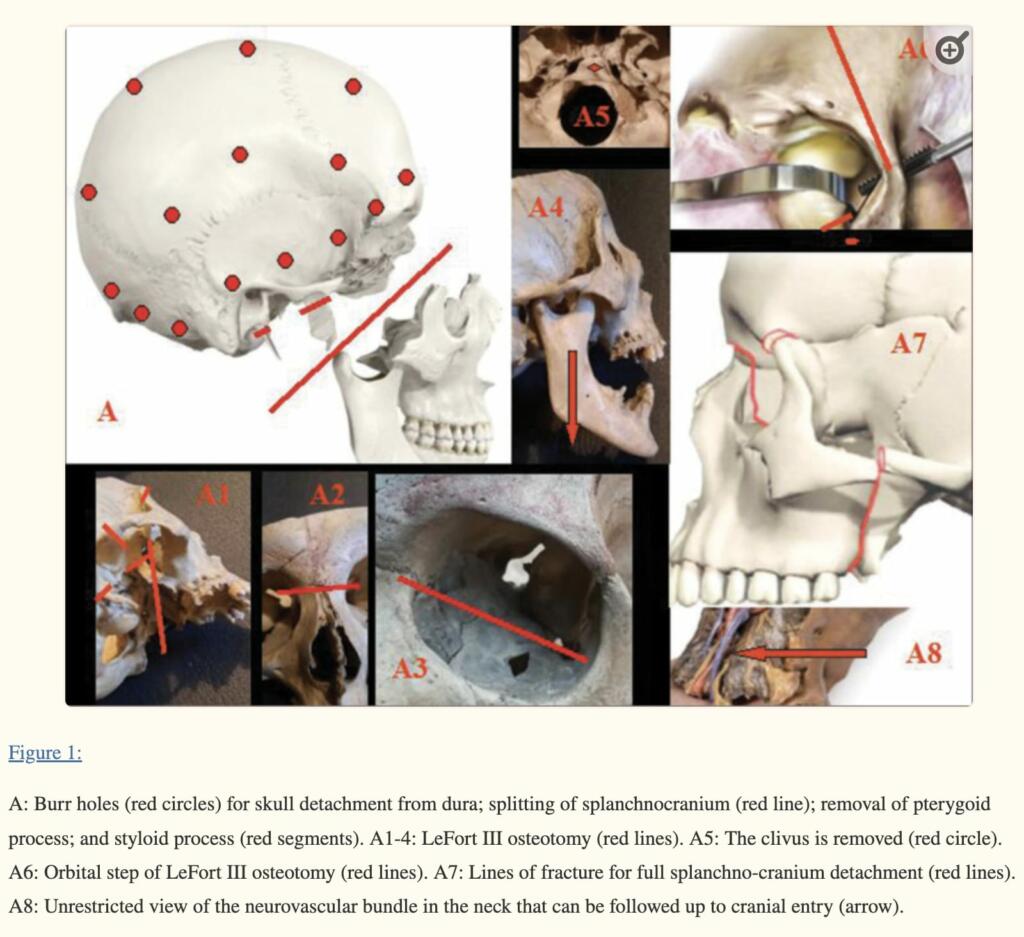
As R’s brain encased in its dura (hypophysis included) is being freed from the cranial vault and base, a robotic scoop with retractable tines is brought into the operating field. This envelops the brain and supports it as the dural detachment proceeds, and facilitates the final transfer onto D.

Vascular Reconnection
BRAVE requires a rapid restart of the circulation to R’s brain. However, anatomical (in particular, the highly constrained surgical space of the cranial fossae) and technical considerations[3] rule out standard manual sutured anastomosis of neurovascular structures. Instead, BT exploits sutureless vascular anastomosis (SVASTOM).
A pretransplant angiography in both R and D is mandatory to assess the entire vasculature, including anatomic variations.
Cranial Nerve Reconnection
Similarly to vascular reconnection, sutured anastomosis is ruled out for cranial nerve reconstruction. Besides the constrained operative space, microsuturing cannot reestablish cranial nerve function rapidly, being exclusively dependent on regeneration. In addition, microsuturing is traumatizing to the nerve (reviewed in De Medinaceli). It goes without saying that BT is acceptable exclusively under condition that rapid recovery of neural transmission ensues. The patient is expected to emerge from post transplant-induced coma with cranial nerve function already present or rapidly recovering. Neural fusion (NF) and sutureless nerve anastomosis (SNATOM) aim at solving this problem. NF would reestablish immediate transmission of electrical impulses, while SNATOM firms up the coaptation.
Importantly, R’s and D’s cranial nerves are severed beyond the actual point of final connection so that any Wallerian degeneration that usually starts within minutes of section is offset by severing the initially degenerating extra-length once the brain has been placed on D’s skull base and fusion initiated (see in Canavero and Ren).
Rodent studies show that, at least for healthy sciatic nerves, stretching up to 30% is not harmful: this is important for surgical maneuvering .
All cranial nerves have less than 100,000 axons each, with the optic nerve being the outlier (1,200,000 fibers).
Unless performed in a clone, variation of the diameter of cranial nerves must be assessed with high-resolution MRI before BT in D.

Brian Wang is a Futurist Thought Leader and a popular Science blogger with 1 million readers per month. His blog Nextbigfuture.com is ranked #1 Science News Blog. It covers many disruptive technology and trends including Space, Robotics, Artificial Intelligence, Medicine, Anti-aging Biotechnology, and Nanotechnology.
Known for identifying cutting edge technologies, he is currently a Co-Founder of a startup and fundraiser for high potential early-stage companies. He is the Head of Research for Allocations for deep technology investments and an Angel Investor at Space Angels.
A frequent speaker at corporations, he has been a TEDx speaker, a Singularity University speaker and guest at numerous interviews for radio and podcasts. He is open to public speaking and advising engagements.
It is not merely re-connecting a cranial nerve that is the challenge. Those of us involved in surgery of the skull base can tell you about a phenomenon called Aberrant Regeneration, most often encountered after Bell’s Palsy or after facial nerve neurorrhaphy in which a severed facial nerve is re-connected.
In Bell’s Palsy, the nerve that moves the face swells within its bony canal and chokes its axons off, which die back to the brainstem and, after a period of time begin to grow back seeking the motor end plates of the face which they innervate. Trouble is, they get lost on the way. So an axon that started out life innervating the corner of the lip may regenerate to now innervate the eyelid muscles. The patient goes to smile, and their eye closes involuntarily. Branches of the facial nerve also go to the lacrimal and salivary glands, and aberrant regeneration of these divisions leads to “crocodile tears”: you smell something delicious and tears start rolling down your cheeks because those pathways are trying to salivate.
Grossly anastomosing 24 cranial nerves with SNATOM would not solve this problem of cross-wiring. We can easily grasp the disability which it causes in the case of the facial nerve; now apply it to nerves like the vagus or the optic nerve and you can see that you have a major technological problem to solve beyond just plug and play.
You arent growing a body without a brain. You need hormones and they need a feedback loop
This makes the head transplant look easy
Why isn´t it anyone commenting on this part?
“1. Rejuvenate the body by growing a body using an egg cell gene edited to not grow the brain”
Yes, transplanting a brain is far beyond our technology right now.
But GROWING ENTIRE BODIES, WITHOUT BRAINS, FROM EGG CELLS, is ALSO beyond our technology.
Ah, actually, that’s the easy part.
It is’t. The brain contains. Among other things, the putuitary and hypothalamus. I doubt artificial hormones with no feedback will work
That’s STILL the easy part of this. You don’t need literally no brain, with literally no brain you’d have no spinal cord, either. What you actually need is a very minimal brain with no frontal lobes. There are several birth defects like that which you’d ‘just’ have to artificially recreate.
I say it’s the easy part because accomplishing that is straightforward compared to doing the surgical portion and not ending up with a blind paraplegic.
The hardest part of producing the bodies?
Defending against the enraged mobs, actually.
There seems to be a certain lack of imagination here. For instance, why would you not perform the transfer in an isotonic fluid bath, to spare the brain gravitational stresses?
But the chief thing that occurs to me is that the detailed arrangement of axons in a large nerve isn’t determinant in detail; Just butt one cut end against another, and you’ll get SOME degree of functionality, but a lot of connections would be scrambled. Eventually you might relearn what goes to what, I suppose, at least for sense of touch, but for sight? I doubt it.
This is not the sort of procedure that can successfully done with such gross operations. Unless by success you just mean that the patient lives, and nothing more. It’s going to require something approaching nanotechnology, to sort things out. The new body will have to be cultivated to have matching ‘wiring’ and circulatory system. You probably want to create in place a kind of quick disconnect system, so the actual transfer takes place in minutes, not hours.
Conceptually brain transplant IS the way to go for whole body rejuvenation, but we don’t remotely have the tech now to pull it off without the result being a horror show. And the proposed brain rejuvenation surgery is even worse.
Integrating cutting-edge technologies such as brain-machine interfaces (BMIs), cloned organs, and dialysis into a whole brain transplant procedure requires a multidisciplinary approach. Here’s how these technologies could be utilized:
Brain-Machine Interfaces (BMIs): These interfaces could be instrumental in establishing functional connections between the transplanted brain and the recipient’s body. BMIs can decode neural signals from the brain and translate them into commands to control prosthetic limbs or other assistive devices. In the context of a brain transplant, they could help bridge gaps in neural communication, facilitating muscle control and sensory feedback. For example, if the neural pathways responsible for motor control are not immediately functional post-transplant, BMIs could be used to interpret brain signals and activate muscles or prosthetic limbs, thus compensating for temporary or permanent deficits.
Cloned or Artificial Organs: Given the complexity and length of a brain transplant procedure, the body’s organs might undergo significant stress or failure. Cloned organs, grown from the recipient’s own cells, could be used to replace failing organs, thus reducing the risk of immune rejection. Artificial organs, such as bioartificial livers or kidneys, could temporarily take over the functions of natural organs, maintaining metabolic balance and removing toxins from the body. This would be particularly crucial during the transplant and recovery phases, where the body’s normal homeostatic mechanisms might be compromised.
Dialysis and Other Supportive Therapies: These therapies would be essential to maintain homeostasis during the transplant process. Dialysis can manage waste products and excess fluids in the body when the kidneys are not functioning optimally, which might be a risk during such an invasive procedure. Other supportive therapies could include artificial ventilation, nutrient and medication administration through intravenous therapy, and continuous monitoring of vital signs to swiftly address any physiological imbalances or complications.
The integration of these technologies would require not only advanced surgical techniques but also robust systems for real-time monitoring and control, sophisticated algorithms for signal processing in BMIs, and a deep understanding of immunology and regenerative medicine. It’s a symphony of medical technology, each component playing a critical role in ensuring the success of such a groundbreaking procedure.
Implementing these solutions before the transplant to enable a seamless, machine-to-machine transfer involves several steps:
Pre-Transplant Conditioning with BMIs: The recipient’s brain could be trained to use brain-machine interfaces prior to the transplant. This training would involve learning to control prosthetic limbs or other devices through neural signals. Establishing this connection pre-transplant means that post-transplant, the brain is already adapted to using BMIs for controlling bodily functions.
Modular Organ Systems: Develop modular cloned or artificial organ systems that can be easily integrated into the recipient’s body. These systems would be designed to quickly connect with the recipient’s vascular and nervous systems, allowing for immediate functionality post-transplant.
Automated Surgical Systems: Utilize advanced robotic surgery systems for precision and consistency. These systems would be programmed to perform specific tasks like vascular and neural connections, making the process more standardized and repeatable.
Seamless Data Transfer: Establish a protocol for seamless data transfer between the recipient’s brain and the medical machines. This would involve sophisticated algorithms and neural interfaces to ensure continuous monitoring and adjustment of bodily functions during the transfer.
Machine-to-Machine Coordination: Implement a system where the surgical machines and support systems (like dialysis and artificial organs) communicate with each other. This inter-machine communication ensures a coordinated approach to maintaining homeostasis and performing the transplant procedure.
transhumanism is the future of mankind. all hail the cybermen.
How’d you like to be the first volunteer?
I’m sure there will be very little pain involved – I mean, a simple knee replacement, with so few nerve fibers disturbed, only hurts like hell for 6 months. Imagine how easily the pain can be ignored when it’s just a few hundred thousand nerves feeding into the largest pain center in the body.
My concept is that it starts with an in situ spinal interface similar to a neuro link but instead of in the brain, it is in the tertiary nervous system. So this allows people who have lost a limb to replace it. Then you move to the core. Core initial volunteers will be people with life-threatening illnesses with little time to live. The recovery will be much simpler if you use bmi on the spinal cord I don’t think it makes sense to cut the brain the way they suggest way more connections to replace. You need to have full control of the nervous system BEFORE severing. That way pain is limited to the nervous system machine interface (NSMI) “just coined that”. Once the nervous system interface is stable you then can amputate those sections and then move to the higher-level systems. This could even be a cure for cancer. Growing clone organs and bodies is key as well. This is doable now with a few hundred million startups. You test animals. Then monkeys. Then amputees. Once you master the NSMI everything else will flow. This allows repeated replacement. Brain core to NSMI, then control structures. Control structures will be various. From space ships to mail sorting, and jet planes to ambulant body units. Organic and not. Humanoid and not. This applies and is desirable to victims of disease and injury today. AI powering the NSMI is another key.
This is vastly more difficult than they make it sound. It isn’t just reconnecting a spinal cord. It’s reconnecting to the retinas and inner ear and muscles and skin in the face. And it isn’t even known whether an adult brain has the plasticity needed to learn a new retina, after being connected.
I find it hard to imagine doing all that without advanced nanotech. And if we had such nanotech, the operation would probably be very different from how it’s described above. It might not even include connecting nerves to nerves. It might involve connecting nerves to nanomachines on both sides, and then having a very simple connection from nanomachines to other nanomachines during the transplant.
But that’s FAR from being possible now. And, as others here have said, the trial and error process to get it working might be truly horrifying.
It is vastly difficult. They are talking about a team of surgeons working for about ten hours. Eventually this would require advanced robotic surgery to make it faster, safer, reliable and affordable.
Yes, far from possible NOW. But is it more possible that other approaches to radical life extension? Could it be perfected?
I agree that brain-to-machine interface the interface would handle blood pumping and neurons and would be connected and grown into the client in situ and transfer would come after the interface heals. would make this transplant more doable morally and physically. would also allow you to be transplanted into the matrix or a robot body or spaceship or whatever too. just need artificial or cloned parts running everything. we are less than 1000 years away from this. with ai possibly less. im going to go scurry off to chat gpt to ask it how lol
While reading this article, all I could think about was Dr. Hannibal Lecter.
Please don’t advocate turning horror movies into reality.
Respect the limits of humans and humanity.
Stop the doctors and scientists who cannot respect those limits.
The line of ethics and morality has been crossed long time ago, but the above also crosses the line of the demonic.
This trans-humanist movement must be stopped.
They are actual monsters and do not realize it.
My suspicion is we had a large survey of races that reached our level of whatever we want to call it and then kept developing, we would find that, almost without exception, they begin taking over their own evolution. That would mean it is not some unnatural process at all, but a perfectly natural one. If one is religious one could even infer that this is the way we are intended to go.
After all, if God didn’t intend us to practice genetic engineering, he wouldn’t have made all the code open source.